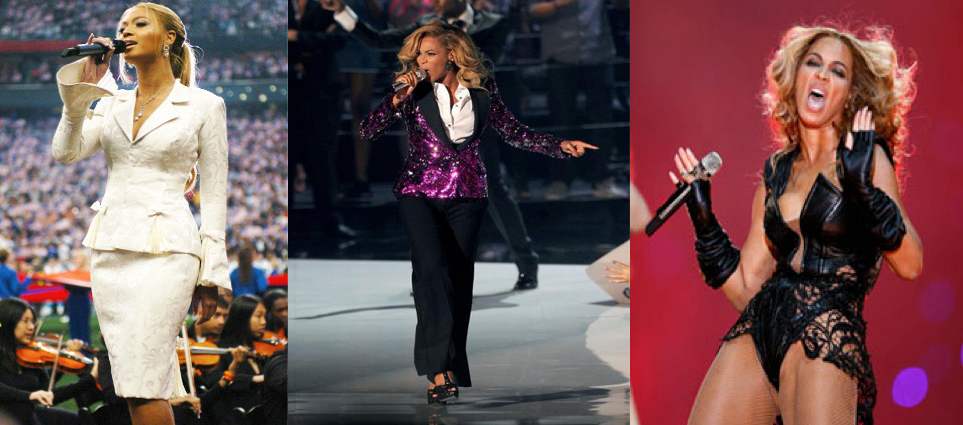
Photo shows Beyonce left 2004 Super Bowl, middle 2012 baby bump announcement, right 2013 Super Bowl
Dear Beyonce, this is a Girl to Girl note.
I have always admired your amazing
voice and have liked your music dating all the way back to Destiny’s
Child. You have come a long way and will go even farther but I do think
it's time you considered "taming the flames of Sasha." I
want you to know that I wish you great success in all your future endeavors,
but there is something I really want you to keep in mind, especially now that
you’re a 31-year old mother.
I want to take you back in time for
a moment and tell you about the time I was in my late teens and early
twenties. The great female pop-culture icon in my day was Madonna.
She had some of the greatest songs, wore the coolest clothes, did the craziest
things and more than anything, she didn’t give a damn about what people really
thought of her. By the way, today, I don’t think that is such a great
thing anymore, but back then I thought it was “cool.”
I absolutely loved Madonna and for
me she was someone I idolized. I began to dress like her, wearing corsets
and leather jackets with crosses and pearls. I smoked cigarettes like
her, danced alone at clubs like she did in her videos, and made myself into
this “untouchable sexual revolutionary” like Madonna was, and still is
today.
Madonna made marriage into a sport
and having a daughter into a hobby. Today, her daughter smokes just like
she does, which brings me to my point.
Your performance at the SuperBowl
looked like you worked very hard. The choreography was fabulous, you and
your dancers and band mates looked amazing, but quite honestly; was it really
necessary to flash your crotch at the audience and at the cameras? Little
children and senior citizens watch the Super Bowl and I’m pretty sure not
everyone wanted to see you flash your coochie at the camera.
I loved your outfit, but thought now
that you’re a mom, shouldn’t you be wearing pants or maybe shorts? I
mean, you just had your baby and I remember how great you looked in that sequin
jacket and the long pants when you first showed off you baby bump. I
thought that outfit showed you have class.
Personally, I like to see you doing
things your way but I also think there’s a time and place for everything.
By the way, I no longer emulate Madonna today and I don’t look back at my
behavior back then with fond memories of idolizing such a socially
irresponsible woman. As a matter of fact, I think I was rather foolish to
think I had any of her qualities. I think as one of the great female
icons out there, you have an opportunity to guide young women who are watching
very carefully what you do.
They watch what you wear, how you
do your hair, your nails, how you move, where you go and who you go with.
They watch who your husband is and how he treats you and they look at who he
was before he married you and what he was about back then. It is
important that you realize you have the power to help him be a more classy icon
as well, if you lead like a lady. To your credit, at least since he's
married you and now has a daughter, he has promised not to refer to women a
"bitches and ho's" anymore in his music. I guess we can all thank
God for that.
I do think if you keep on
performing like you were twenty years old when in fact you are now a 31-year
old mom, you might end up like Madonna. Which isn’t bad, Madonna still
rocks, but is that what you want? I look back to the time you sang
the National Anthem at the Super Bowl of 2004. When I think of your
future, that is how I see you. I hope you do too, for the sake of your daughter and all the young women out there who look to you for answers.
Sincerely,
Alexandra